
- What is a Certified Professional Midwife (CPM)?
- Do Licensed Midwives work in hospitals?
- What are the benefits of midwifery care?
- Is home birth safe?
- Why home birth?
- Are there any medical conditions which would prevent me from being able to see a licensed midwife and plan a home birth?
- If I had a previous c-section birth, can I still have a home birth?
- Who is a good candidate for a home birth?
- What if there is a complication?
- What is your hospital transfer rate?
- Do you offer water birth?
- How much do you charge?
- What payment methods do you accept?
- Do you take insurance?
- Can I pay for midwifery care out of my HSA/FSA account?
- Can I pay for midwifery care using a healthshare?
- If I need to transfer to the hospital during labor, do I get a refund?
- If I need to transfer to the hospital, can you still be my care provider?
- Do I need to see a doctor as well if I choose midwife care?
- Where do prenatal appointments happen?
- When do you start prenatal care?
- Do you accept transfers to midwifery care later in pregnancy?
- What can I expect from prenatal care with you?
- Are there any medical conditions that might develop during my pregnancy which would require me to transfer my care to a doctor?
- What can I expect from labor and birth care with you?
- Do you have medications for pain management at a home birth?
- Do I need a doula for my homebirth?
- Can my other children come to my prenatal appointments and birth?
- What supplies do I need for a home birth?
- What can I expect from postpartum care with you?
What is a Licensed Midwife (LM) & Certified Professional Midwife (CPM)?
A Certified Professional Midwife (CPM) is a knowledgeable, skilled, and independent practitioner who has met the standards for certification and passed a written examination set by the North American Registry of Midwives (NARM). The Certified Professional Midwife credential, issued by NARM, is accredited by the National Commission for Certifying Agencies (NCCA), whose mission is to promote excellence in credentialing for practitioners in all occupations and professions. The NCCA accredits many healthcare credentials, including the Certified Nurse-Midwife. The CPM is the only NCCA-accredited midwifery credential that includes a requirement for out-of-hospital experience.
CPMs are trained and credentialed to offer expert care, education, counseling and support to women for pregnancy, birth and the postpartum period, in order to promote a healthy pregnancy, and help them make informed decisions about their own care. In partnership with their clients, Certified Professional Midwives carefully monitor the progress of the pregnancy, labor, birth, and postpartum period and recommend appropriate management if complications arise, collaborating with other healthcare providers when necessary.
CPMs are not doctors, nurses, or nurse-midwives, nor are they trained as such. This means that in they cannot provide medical care in a hospital or write prescriptions.
Do Licensed Midwives work in hospitals?
No, licensed midwives are trained specifically for out-of-hospital births and work in settings such as birth centers or home births. They are not trained as nurses and therefore cannot provide medical care in a hospital. Certified Nurse Midwives, on the other hand, are trained to provide medical care in hospital settings.
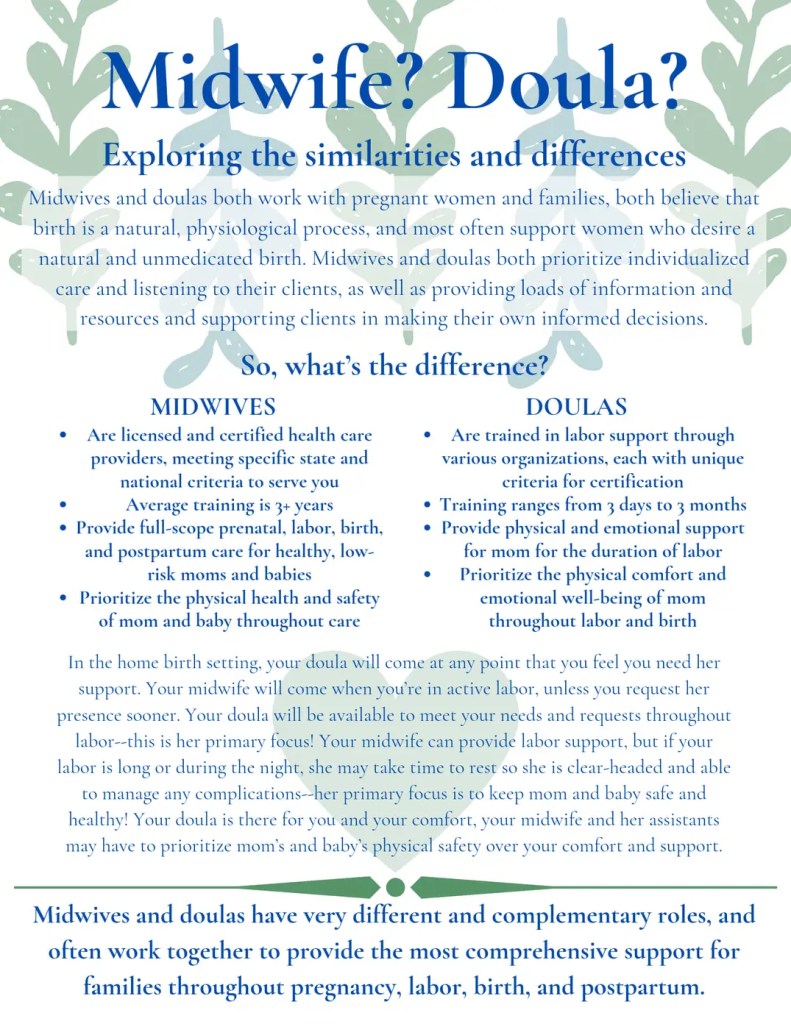
What are the benefits of midwifery care?
Midwives respect childbirth as a natural and sacred process. Our philosophy is fundamentally different to traditional obstetric care, and prioritizes trust in the woman’s body, informed decision-making, and the creation of a caring environment that nurtures both mother and child. Empowerment through education, respecting the mother’s choices, and minimizing unnecessary interventions all contribute to a healthier, more positive birth experience. This collaborative approach ensures that the mother feels supported, heard, and equipped to make decisions that are best for her and her baby. It’s a beautiful vision of maternity care!

As a midwife, I am committed to providing compassionate, woman-centered care. I bring my skills, experience, and heartfelt care, and I see it as both an honor and a responsibility to create a safe, nurturing environment for women on their journey to motherhood. My goal is to support women and families through this transformative time by offering evidence-based information, education, clinical expertise, and guidance. When needed, I provide consultations or referrals to ensure my clients make informed decisions with confidence.
Is home birth safe?
The safety and benefits of midwifery care are well-documented globally, including in the United States. According to World Health Organization statistics, births attended by midwives typically have lower infection rates, fewer cesarean sections, reduced complications, and healthier outcomes, leading to lower overall medical costs compared to physician-attended hospital births. Additionally, there is no difference in infant mortality rates between midwife-attended and physician-attended births for low-risk women. Countries like the Netherlands, Sweden, and New Zealand, which have some of the best birth outcomes in the world, rely on midwives as primary maternity care providers, with approximately two-thirds of babies born at home under midwifery care in these nations.
“Low risk women in primary care at the onset of labor with planned home birth had lower rates of severe acute maternal morbidity, postpartum hemorrhage, and manual removal of placenta than those with planned hospital birth. For parous [at least one prior birth] women these differences were statistically significant. Absolute risks were small in both groups. There was no evidence that planned home birth among low risk women leads to an increased risk of severe adverse maternal outcomes in a maternity care system with well trained midwives and a good referral and transportation system.”
Home Birth Safer Than Hospital Birth: Nation-wide Study Netherlands
According to the Journal of Midwifery & Women’s Health 2013, the C-section rate for low-risk women giving birth in hospitals is approximately 25% versus 6% for those delivering at home or birthing centers in the United States.
The Journal of Midwifery published a study in 2014 called “Outcomes of Care for 16,924 Planned Home Births in the United States: The Midwives Alliance of North American Statistics Project, 2004-2009.” It tracked planned homebirths over a span of six years and revealed an impressive array of evidence supporting the practice as plentifully safe for low-risk moms and their babes, as did the study that came before it, “The CPM 2000 Project,” published in 2005 and examining 5,418 planned homebirths.
Of the 16,924 women planning to give birth at home, fully 89.1% of them accomplished just that. Of the 11% who were taken to the hospital – mostly for trouble progressing – another 4.5% (for a grand total of 93.6%) were yet able to birth spontaneously, while 1.2% managed instrumentally assisted vaginal births and 5.2% birthed by cesarean section. Most babies were born in excellent condition with five-minute APGAR scores of seven or greater.
These stellar results were accompanied by a tremendous measure of client satisfactions and were achieved at a fraction o f what is typically costs for birth to be accomplished inside the American hospital system.
Homebirth: Safe and Sacred by Kim Osterholzer
Home Birth Safety Outcomes – Midwives Alliance of North America (MANA) This study, which examines nearly 17,000 courses of midwife-led care, is the largest analysis of planned home birth in the U.S. ever published.
Why home birth?
Home birth offers many benefits, including autonomy and freedom of movement, choice of birthing positions, and the ability to eat and drink during labor. It also reduces the risk of infection and disease, minimizes complications, and avoids unnecessary exams or interventions. There are no time constraints on labor and birth, allowing for respectful, individualized care with empowering and encouraging support. Home birth fosters trust in your body’s natural ability to give birth, creates a physiologically supportive environment for early bonding and healthy breastfeeding, involves the entire family, and provides a peaceful, private setting free from disruptions and distractions.
The Homebirth Choice – Midwifery Today
There’s No Place Like Home – Midwifery Today

Are there any medical conditions which would prevent me from being able to see a licensed midwife and plan a home birth?
Yes. Medical conditions that may disqualify a woman from planning a safe home birth with a licensed midwife include, but are not limited to, cardiac disease, diabetes, hepatitis B, high blood pressure, substance abuse, blood clotting disorders, and seizure disorders.
If I had a previous c-section, can I still have a home birth?
Yes! At least 75% or more of women who have had a previous C-section can successfully achieve a VBAC (Vaginal Birth After Cesarean). I have supported many successful VBACs both at home. During your consultation, we can explore the risks and benefits of VBAC and assess if you are a suitable candidate for a home VBAC.
I have some information on VBACs on my Resources page.
This is a great article on the truth about uterine rupture via VBAC.com. Visit VBAC.com and VBACfacts.com for more great information.
Who is a good candidate for a home birth?
- Women in generally good health with no pre-pregnancy medical risk factors, and who have a low-risk pregnancy and a healthy baby.
- Women who proactively educate themselves about pregnancy, nutrition, childbirth, home birth, newborn care, and breastfeeding, and who prepare thoroughly for a natural birth.
- Women with a responsible, self-reliant attitude toward their care during pregnancy and labor, and who are prepared to take full responsibility for the outcome of their home birth choice.
- Women who take excellent care of their physical, emotional, and spiritual well-being.
- Women who actively manage their health to remain a low-risk candidate for home birth by eating well, taking quality supplements, engaging in moderate exercise, and avoiding harmful substances like smoking, drugs, alcohol, and toxins.
What if there is a complication?

Studies consistently show that for women with normal, healthy, and uncomplicated pregnancies, planned home birth with a skilled midwife is as safe as, or even safer than, hospital birth. Approximately 90% of births progress normally without complications. However, childbirth involves risks regardless of the setting, and no midwife, no matter how experienced, can guarantee a completely safe home delivery.
I am certified in both adult and infant CPR and am equipped with tools and medications to manage certain rare complications, such as maternal hemorrhage and newborn breathing difficulties. I have experience handling various emergencies. By closely monitoring the well-being of both mother and baby and minimizing unnecessary interventions, many complications can be prevented. Transfers to a hospital typically occur for non-emergency reasons, such as prolonged labor or maternal exhaustion. We will develop a hospital transfer plan by 37 weeks of pregnancy to ensure we are prepared if a transfer becomes necessary.
For more info, please check out: But What if Something Goes Wrong? How Midwives Handle Complications at Homebirths
Complications and Homebirth Midwifery
What is your hospital transfer rate?
Mother, during labor or immediately after birth: 7%
Do you offer water birth?
Absolutely! Laboring or birthing in water can greatly help manage the intensity of contractions. The warmth of the water soothes muscles and joints, while the buoyancy allows for easier movement. My professional-grade inflatable birthing tub is more spacious and comfortable than a standard bathtub, and it fits easily in most rooms, with dimensions of 65″ x 57″. I offer the use of this tub for a small additional fee. You will need to purchase a few extra supplies, including a disposable liner for the tub, a hose, and a faucet adapter.
If you have more questions about water birth, visit the waterbirth.org website.
How much do you charge?
Please feel free to contact me and I would be happy to send you an informational handout detailing the cost of my comprehensive midwifery care and homebirth package, what it includes, optional items that may be added on, and refund policy.
More resources: Affording Homebirth: The Money Aspect of Midwifery Care
10 Ideas for Affording a Homebirth
What payment methods do you accept?
I accept cash, personal checks, Paypal bank transfer, Venmo, Zelle, or Ca$h app. Clients may also use a credit card, however there is a 3.5% processing fee for this option.
Do you take insurance?
Licensed Midwives are not typically contracted (in-network) with insurance companies. Because of this, we are considered out-of-network providers and operate on a self-pay basis.
While some insurance plans may offer partial reimbursement for home birth services, most do not cover care with a Licensed Midwife, or they apply high out-of-network deductibles and co-insurance rates. It is common for out-of-network deductibles to range from $10,000–$15,000, which means families typically receive little to no reimbursement.
For clients who wish to explore their benefits, we offer access to a third-party billing service (for an additional fee). The service can help verify your plan’s out-of-network maternity benefits, advise whether submitting a claim is likely to result in reimbursement, and assist with creating a superbill for you to submit directly to your insurance company after the birth.
The full midwifery care fee is due to Your Taylor Midwife by 34 weeks of pregnancy regardless if clients will be attempting to obtain insurance reimbursement after the birth.

Can I pay for midwifery care out of my HSA/FSA account?
Yes! I can charge an HSA/FSA card in my office, or you can have a check issued directly to me from your account.
Can I pay for midwifery care using a healthshare?
Yes! Each healthshare will have different ways of operating, so you will need to look into your specific healthshare to find out how and when to secure payment. Sometimes it can take a number of months for payment to come in from the healthshare, if that is the case, the client is still responsible to pay according to the payment schedule of $500 non-refundable deposit, and $250 at each prenatal visit.
If I need to transfer to the hospital during labor, do I get a refund?
No. Choosing out-of-hospital midwifery care and planning a community birth does not guarantee a specific birth outcome, a home birth, or even a vaginal delivery.
A midwife’s role is to guide clients toward a safe home birth, and it is also our responsibility to recommend transfer if a situation arises that makes a home birth unsafe for the mother or baby. We use reasonable knowledge and skill to determine whether birth can safely continue at home or if transfer to a medical facility is necessary. As a midwife, my commitment is to provide expert care, support, and guidance throughout pregnancy and birth, always prioritizing the safety and well-being of both the client and their baby. However, childbirth can be unpredictable, and sometimes a transfer of care to a physician or hospital is needed, which may include interventions such as a cesarean. By hiring me, clients are contracting for my time, expertise, and services; not for a guaranteed birth outcome or location.

If I need to transfer to the hospital, can you still be my care provider?
No, licensed midwives are trained specifically for out-of-hospital births and are not doctors, nurses, or nurse-midwives, which means they cannot provide medical care in a hospital setting. However, I will make every effort to accompany clients who require hospital transfer during active labor, assisting with the handoff to the medical team while offering advice, emotional support, and encouragement throughout the process until a care plan is established. Once the mother and baby are discharged from hospital care, I will continue with postpartum care for them.
Do I need to see a doctor also if I choose midwife care?
Unless there are specific medical concerns in your pregnancy that require co-management with a doctor, you don’t need to visit a doctor or OB/GYN office when you choose midwifery care! During your prenatal appointments, I conduct tests such as urine analysis, measure your blood pressure and pulse, listen to the baby’s heartbeat, and more—similar to what is done at a doctor’s office. I also handle all necessary lab work in my office, so there’s no need to go elsewhere for blood draws.
Where do prenatal appointments happen?
All prenatal care except for one home visit in the client’s home at approximately 36 weeks is done at my office here in Taylor, which is conveniently located at approximately highways 79 and 95.

When do you start prenatal care?
It’s important to start looking for a midwife as soon as possible since I have limited spots available for clients with due dates in a specific month. The earlier you reach out, the better the chance of securing an opening around your due date. Typically, mothers contact me to schedule a complimentary consultation soon after receiving a positive pregnancy test. I offer early elective ultrasounds starting at 7 weeks and gender determination bloodwork (SneakPeek) as early as 6 weeks. Your first regular appointment is usually scheduled between 10-12 weeks, when we can often hear the baby’s heartbeat with a handheld Doppler. This allows us to have months of appointments throughout your pregnancy to build a relationship, discuss natural home birth, and ensure the best care for a successful home birth.
Do you accept transfers to midwifery care later in pregnancy?
I often book up early, so availability for late transfer clients may be limited. If I do have an open spot during your due month, I’m happy to arrange a consultation to determine if we could be a good fit for working together towards a home birth. As long as there are no medical concerns, and the mother can provide records of previous care, is confident and knowledgeable about home birth and midwifery care, and is willing to take responsibility for her home birth choice, I’m open to considering a transfer of care later in pregnancy.
What can I expect from prenatal care with you?
My prenatal care schedule includes appointments every 4 weeks until 28 weeks, every 2 weeks from 28 to 36 weeks, and weekly until birth. Prenatal care involves monitoring the baby’s growth, listening to the heartbeat, checking maternal vital signs, performing necessary lab work, providing nutritional and herbal guidance, and assessing the mother’s physical and emotional well-being. We’ll also discuss resources for preparing for a natural labor and birth, and collaborate with or refer to other healthcare providers if needed. Evidence-based research and information on prenatal and newborn procedures will be provided to help clients make informed decisions.
Each appointment lasts 30-60 minutes, giving ample time for questions, meaningful discussions, and addressing any fears or concerns the client or her family may have. This personalized care fosters a trusting relationship, helping the mother approach labor and birth with confidence, safety, and peace of mind.

Are there any medical conditions that could arise during pregnancy which would require me to transfer care to a doctor?
Yes. Medical conditions that may disqualify a mother from attempting a homebirth with a licensed midwife in Texas and require transfer of care to a qualified healthcare provider (per Texas Admin. Code TAC §115.114) include, but are not limited to: gestational diabetes requiring medication, hypertension or preeclampsia, anemia unresponsive to treatment, suspected fetal growth restriction, oligohydramnios or polyhydramnios, placenta previa, baby not in head-down position at term, multiple gestation, a known significant fetal anomaly, active genital herpes, ruptured membranes without labor, preterm labor or rupture of membranes before 37 weeks, post-dates pregnancy beyond 42 weeks, or any other condition or symptom that could threaten the health or life of the mother or baby.
What can I expect from labor and birth care with you?
In the weeks preceding birth, we discuss signs that can indicate labor may be coming. I stay in close contact with the mother and/or her support person during early labor, and together we decide the best time for me to join them at home once she is in active labor. Upon arrival, I help create a calm, peaceful, an undisturbed atmosphere. My role is to offer empowering support, suggestions, and trust in the mother’s natural ability to give birth. Throughout labor, I discreetly monitor the well-being of both mother and baby, while allowing the birth to progress naturally at its own pace. I maintain a hands-off, non-interventive approach while staying attentive and available for support or encouragement.
If needed, I may suggest different activities or positions, like taking a walk or kneeling, to help labor along. In the comfort of her home, the mother often feels more at ease to try various labor positions and move freely. I also encourage her to eat or drink as she is able to sustain her energy. When the time comes for delivery, she is free to give birth in whatever position feels most natural and comfortable to her. Comfort measures available in the home include massage, hydrotherapy, relaxation techniques, breathing exercises, visualization, position changes, heat/ice application, acupressure, herbs, essential oils, and homeopathic remedies.

After the birth, I assess the newborn’s APGAR score and perform a full examination, including checking weight, length, reflexes, and ensure breastfeeding is established.

I also monitor the mother’s vitals, check for any tears and suture if needed, assist her with showering if she wishes, and prepare something nourishing for her to eat and drink. Before my assistant and I leave, usually 2-3 hours after birth, we make sure both mother and baby are happy, healthy, and stable. We’ll provide any final instructions, help settle the family into bed for some well-earned rest, clean up, start the laundry, and quietly see ourselves out.
Check out the Resources page for some beautiful videos which share a glimpse of what a typical homebirth is like!
The Homebirth Choice – Midwifery Today.
Do you have medications for pain management at a home birth?
Licensed midwives are trained to offer non-pharmacological pain relief methods, such as hydrotherapy, breathing techniques, massage, and positioning to help manage labor pain. For more advanced pain relief options, like epidurals or systemic analgesics, you would need to be in a hospital setting.
Do I need a doula for my homebirth?
A doula is a vital member of the birth team! For first-time mothers or those having a primary VBAC (vaginal birth after cesarean), I strongly recommend hiring a doula for labor support. First-time moms and primary VBACs often experience longer labors, and a doula’s continuous support and guidance have consistently been shown to significantly impact the birth experience and outcome. While a midwife focuses on the medical safety of both mother and baby, a doula provides emotional and physical support throughout labor. In the event of a transfer to a hospital, having a doula who understands your birth preferences and can communicate and coordinate with hospital staff is incredibly valuable.
More info on the role of doulas on my Resources page
Can my other children come to my prenatal appointments and birth?
Absolutely! Siblings are welcome at all prenatal visits and during the home birth. I have a toy basket in my office to keep children entertained while we meet. If you choose to have your other children present at the birth, please ensure that you have a reliable caretaker (not your partner) at home who is solely responsible for caring for them, allowing you and your partner to focus on the delivery. Beyond that, you are free to include anyone else you wish. The key is that you feel completely comfortable and at ease with everyone present, as this can greatly influence your birthing experience.

6 Birth Videos to Prepare Siblings
Inviting Your Older Kids to Your Upcoming Homebirth
What supplies do I need for a home birth?
It’s quite simple! You’ll order my custom birth kit 34 weeks. If you’re planning a water birth with one of my inflatable tubs, there are a few additional items to include. The birth kit, along with a stack of towels, washcloths, and an extra set of sheets, covers everything you’ll need. Many people are surprised by how minimal the mess is during a home birth.
The birth kit includes disposable waterproof underpads (“Chux” pads) and a plastic shower curtain to protect surfaces like the bed and carpet. These items are disposed of after the birth. We’ll handle the cleanup by gathering all trash and laundry, and I or my assistant can start the laundry before we leave, if you’d like. We also ensure that everything is tidied up so you won’t have to worry about the cleanup.
What can I expect from postpartum care with you?
- In-home visits during the first two weeks after birth to assess healing, answer questions, and support feeding, newborn weight gain, and baby care
- Office appointments from weeks 2–6, with ongoing check-ins as needed
- Phone and text availability for questions, concerns, or reassurance during the 6 week period
- Newborn screenings, including tests for congenital heart defects and metabolic conditions
- Breastfeeding support, and referral to lactation consultant for further support if needed
- Completion and filing of the birth certificate and coordination of other newborn paperwork
- We ensure a smooth transition of care to a pediatrician, and connect families with local resources for feeding, sleep, pelvic floor therapy, perinatal mental health, and infant care
Every mother deserves to feel supported—physically, emotionally, and practically—as she heals and adjusts to this new season of life.
Still have questions?
Get in Touch, Call/Text the Office Line (913) 283-5768, or Email me.
